4.2 Types of Nonverbal Communication
Learning Objectives
- Define kinesics.
- Define haptics.
- Define vocalics.
- Define proxemics.
- Define chronemics.
- Provide examples of types of nonverbal communication that fall under these categories.
- Discuss how personal presentation and environment provide nonverbal cues.
Just as verbal language is categorized in various ways, there are also different types of nonverbal communication. As we learn about each type of nonverbal signal, remember that nonverbals often work together, combining to repeat, modify, or contradict the verbal message.
Kinesics
Kinesics comes from the root word kinesis, which means “movement” and refers to the study of hand, arm, body, and face movements (Harrigan, 2005). Specifically, this section will outline gestures, head movements and posture, eye contact, and facial expressions as nonverbal communication.
Gestures
There are three main types of gestures: adaptors, emblems, and illustrators (Andersen, 1999). Adaptors are touch behaviours and movements that indicate internal states typically related to arousal or anxiety. Adaptors can be targeted toward the self, objects, or others. In regular social situations and healthcare environments, adaptors result from uneasiness, anxiety, or a general sense that we are not in control of our surroundings. Many of us subconsciously click pens, tap our feet, or engage in other adaptors during classes, exams, meetings, or while waiting as a way to do something with our excess energy. If you were to watch yourself on video recordings (most students have to do this for exams or assignments), you would likely notice nonverbal adaptors you did not know you used. In stressful situations, people most commonly use self- or object-focused adaptors. Common self-touching behaviours such as scratching, twirling hair, or fidgeting with fingers or hands are considered self-adaptors. Some self-adaptors manifest internally, such as coughs or throat-clearing sounds. Other people play with dry-erase markers, their note cards, the change in their pockets, or the lectern while speaking. The use of object adaptors can also signal boredom as people play with the straw in their drink or peel the label off a bottle of beer. Smartphones have become standard object adaptors, as people can fiddle with their phones to help ease anxiety.
Emblems are gestures with a specific agreed-upon meaning often bound by culture. These are different from the signs used by hearing-impaired people or others who communicate using sign language: even though they have a generally agreed-upon meaning, they are not part of a formal sign system such as American Sign Language that is explicitly taught to a group of people. A hitchhiker’s raised thumb, the “OK” sign with thumb and index finger connected in a circle with the other three fingers sticking up, and the raised middle finger are all examples of emblems with an agreed-upon meaning or meanings within a culture. Emblems can be still or in motion; for example, rolling your hands over and over in front of you says, “Move on.”

Just as we can trace the history of a word or its etymology, we can also trace some nonverbal signals, especially emblems, to their origins. Holding up the index and middle fingers in a “V” shape with the palm facing in is an insulting gesture in Britain that means “up yours.” This gesture dates back centuries to when the primary weapon of war was the bow and arrow. When archers were captured, their enemies often cut off these two fingers, which was seen as the ultimate insult and worse than being executed since the archer could no longer shoot his bow and arrow. So holding up the two fingers was a provoking gesture used by archers to show their enemies that they still had their shooting fingers (Pease & Pease, 2004, p. 121).
Illustrators use the most common gestures to illustrate the verbal message they accompany but cannot stand independently (Adler et al., 2021). For example, you might use hand gestures to indicate the size or shape of an object. Unlike emblems, illustrators do not typically have meaning and are used more subconsciously than emblems. These largely involuntary and seemingly natural gestures flow from us as we speak but vary in intensity and frequency based on context. Although we are never explicitly taught how to use illustrative gestures, we do it automatically. Think about how you gesture when having an animated conversation on the phone even though the other person can not see you, or how you verbally give instructions and directions to a client, but as you do so, you use your arms and fingers to point (Adler et al., 2021).
Head Movements, Posture, and Positioning
Head movements and posture are grouped because both are often used to acknowledge others and communicate interest or attentiveness. Regarding head movements, a head nod is a universal sign of acknowledgment in cultures where the formal bow is no longer used as a greeting. In these cases, the head nod essentially serves as an abbreviated bow. An innate and universal head movement is the headshake back and forth to signal “no.” This nonverbal signal begins at birth, even before a baby knows it has a corresponding meaning. Babies shake their heads side to side to reject their mother’s breast and later reject attempts to spoon-feed (Pease & Pease, 2004, p. 232). This biologically based movement then sticks with us to become a recognizable signal for “no.” We also move our heads to indicate interest. For example, a head-up typically indicates an engaged or neutral attitude, a head tilt indicates interest and is an innate submission gesture that exposes the neck and subconsciously makes people feel more trusting of us, and a head down signals a hostile or aggressive attitude (Pease & Pease, 2004, p. 233).
There are four general human postures: standing, sitting, squatting, and lying down (Hargie, 2011). Each posture has many variations, and when combined with particular gestures or other nonverbal cues, they can express many different meanings. Most of our communication occurs while we are standing or sitting. One interesting standing posture involves putting our hands on our hips and is a nonverbal cue that we use subconsciously to make us look bigger and show assertiveness. When the elbows are pointed out, this prevents others from getting past us quickly and is a sign of attempted dominance or a gesture that says we are ready for action. While sitting, leaning back shows informality and indifference, straddling a chair is a sign of dominance (but also some insecurity because the person is protecting the vulnerable front part of their body), and leaning forward shows interest and attentiveness (Pease & Pease, 2004).
Nonverbal communication can help communicate emotions such as empathy, compassion, and acceptance. It is often how health care providers respond rather than what they say that leaves a lasting impression on clients, so it is essential to be aware of how you communicate using nonverbal behaviours. Nonverbal behaviours must align with your verbal behaviours so clients understand what you are saying clearly. For example, it would be confusing for the client if you had a sombre tone of voice, a distancing posture, and avoided eye contact while attempting to maintain a therapeutic relationship with the client. Try to ensure positioning where you are both at the same vertical level and at a slight angle toward one another. This positioning conveys an open and non-confrontational, and nonauthoritative space. Avoid standing over the client if they are sitting or lying in bed whenever possible. It is better to sit down, which also conveys that you have time to listen to them. There are many models to inform your nonverbal communication. One helpful model is Stickley’s SURETY model (2011), which stands for:
S- Sit at an angle to the client. This is a non-confrontational position. Please remember that each client has their definition of personal space, so watch for signs of discomfort and respond accordingly. U– Uncross legs and arms. Crossing our legs and arms may communicate defensiveness or disinterest in what a client says. Deliberately uncrossing our legs and arms communicates that we are open to hearing what the client says. We must be careful that this position does not lead to slouching as this position is too open within a professional environment. R- Relax. This position may take some practice to become comfortable. A health professional needs to become comfortable listening in this position. E- Eye contact. Appropriate eye contact can be a powerful way of communicating with a client. It demonstrates respect, presence and active listening. Appropriate eye contact occasionally breaks, thus ensuring a health professional does not stare at a client, which can be perceived as threatening, intrusive and intimidating. Appropriate eye contact is not universal, and we must consider the influence of age, gender, culture and medical or abuse history. T- Touch. Appropriate use of touch is not universal. We must be sensitive to touch (purpose) while considering context and the influence of age, gender, culture, and client history. Using touch respectfully conveys caring, empathy and understanding. Touch can also be considered abusive when misused. Health professionals use touch when conducting assessments, transferring patients, and during bedside treatments and procedures. The therapeutic use of touch is not straightforward and should be guided by professional organizations’ standards of practice and institutional or business policies. Y- Your intuition. Health professionals gain confidence with practice and should begin to trust their intuition. One’s use of intuition is dependent on their culture, belief, and personal and professional lived experiences.
Body Language
Body language affects how others see us but may also change how we see ourselves. The following video explains how Social psychologist Amy Cuddy, views “power posing” — standing in a posture of confidence, even when we do not feel confident — can affect testosterone and cortisol levels in the brain and might even impact our chances for success.
Watch: Amy Cuddy: Your body language may shape who you are
Video Transcript (see Appendix B 4.2)
Eye Contact
We also communicate through eye behaviours, primarily eye contact. While eye behaviours are often studied under the category of kinesics, there is a specific branch of nonverbal studies called oculesics, which comes from the Latin word oculus, meaning “eye.” The face and eyes are the main points of focus during communication, and along with our ears, our eyes take in most of the communicative information around us. The saying “The eyes are the window to the soul” is accurate in terms of where people typically think others are “located,” which is right behind the eyes (Andersen, 1999). Certain eye behaviours have become tied to personality traits or emotional states, as illustrated in phrases like “hungry eyes,” “the evil eye,” and “bedroom eyes.”
Eye contact serves several communicative functions, from regulating interaction to monitoring interaction, conveying information, and establishing interpersonal connections. Regarding regulating communication, we use eye contact to signal to others that we are ready to speak or cue others to speak. We have all been in that awkward situation where we are asked a question, no one else responds, and the speaker looks directly at us as if to say, “What do you think?” In that case, eye contact is used to cue us to respond. During an interaction, eye contact changes as we shift from speaker to listener. Canadians typically shift eye contact while speaking — looking away from the listener and then looking back at their face every few seconds. Toward the end of our speaking turn, we make more direct eye contact with our listener to indicate that we are finishing up. While listening, we tend to make more sustained eye contact, not glancing away as regularly as we do while speaking (Martin & Nakayama, 2010, p. 276).
Aside from regulating conversations, eye contact is also used to monitor interaction by taking in feedback and other nonverbal cues and sending information. Our eyes bring in the visual information we need to interpret people’s movements, gestures, and eye contact. Speakers can use eye contact to determine whether an audience is engaged, confused, or bored and then adapt their message accordingly. Our eyes also send information to others. People know not to interrupt when thinking deeply because we naturally look away from others when processing information. Making eye contact with others also communicates that we are paying attention and are interested in what another person is saying. Eye contact is a crucial part of active listening.
Eye contact can also be used to intimidate others. Depending on the region of the world, there are social norms about how much eye contact we make with people, and those norms vary depending on the setting and the person. Staring at another person in some contexts could communicate intimidation, while in others, it could communicate flirtation. As we learned, eye contact is a crucial immediacy behaviour, and it signals to others that we are available for communication. Once communication begins (if it does), eye contact helps establish rapport or connection. We can also use our eye contact to signal that we do not want to make a connection with others. For example, in a public setting such as an airport or a gym where people often make small talk, we can avoid making eye contact to indicate that we do not want to talk with strangers. Another person could use eye contact to try to coax you into speaking. For example, when one person continues to stare at another person who is not reciprocating eye contact, the person avoiding eye contact might eventually give in, become curious, or become irritated and say, “Can I help you with something?” Eye contact sends and receives essential communicative messages that help us interpret others’ behaviours, convey information about our thoughts and feelings, and facilitate or impede rapport or connection. This list reviews the specific functions of eye contact:
- regulate interaction and provide turn-taking signals
- monitor communication by receiving nonverbal communication from others
- signal cognitive activity (we look away when processing information)
- express engagement (we show people we are listening with our eyes)
- convey intimidation
- express flirtation
- establish rapport or connection
Facial Expressions
Our faces are the most expressive part of our bodies. Think of how photos are often intended to capture a particular expression “in a flash” to preserve for later viewing. Even though a photo is a snapshot in time, we can still interpret much meaning from a human face caught in a moment of expression. Basic facial expressions are recognizable by humans worldwide. Much research has supported the universality of a core group of facial expressions: happiness, sadness, fear, anger, and disgust. The first four are especially identifiable across cultures (Andersen, 1999). However, the triggers for these expressions and the cultural and social norms that influence their displays are culturally diverse. If you have spent much time with babies, you know they can express all these emotions. Seeing the pure and innate expressions of joy and surprise on a baby’s face makes playing peek-a-boo entertaining for adults. As we get older, we learn to follow display rules for facial expressions and other signals of emotion and to control our emotional expression better based on our culture’s norms.
Smiles are powerful communicative signals and are a vital immediacy behaviour. Although facial expressions are typically viewed as innate, and several are universally recognizable, they are not always connected to an emotional or internal biological stimulus; they can serve a more social purpose. For example, most of our smiles are primarily made for others and are not simply an involuntary reflection of an internal emotional state (Andersen, 1999). However, these social smiles are slightly but perceptibly different from more genuine ones. People generally perceive smiles as more genuine when the other person smiles “with their eyes.” This type of smile is difficult to fake because the muscles around the eye activated when we spontaneously or genuinely smile are not under our voluntary control. These muscles’ involuntary and spontaneous contraction moves the skin around our cheeks, eyes, and nose to create a smile distinct from a fake or polite smile (Evans, 2001, p. 107). People can distinguish the difference between these, which is why photographers often engage in cheesy joking with adults or use props with children to induce a genuine smile before they snap a picture.
Facial expressions help set the emotional tone when speaking in front of others. To set a positive tone before speaking, briefly look at the audience and smile to communicate friendliness, openness, and confidence. Beyond opening and welcoming facial expressions, facial expressions communicate a range of emotions and can infer personality traits and make judgments about a speaker’s credibility and competence. Facial expressions can communicate that a person is tired, excited, angry, confused, frustrated, sad, confident, smug, shy, or bored. For example, a face with little animation may make a patient or client think you are bored with what they say. It is also essential that facial expressions match what is being said. A smile, bright eyes, and slightly raised eyebrows will nonverbally enhance the verbal message when delivering something light-hearted or humorous. When delivering something severe or sombre, a furrowed brow, a tighter mouth, and even a slight head nod can enhance that message. If your facial expressions and speech content are inconsistent, the mixed messages could confuse clients and families, leading them to question your credibility.
Haptics
Think about how touch can comfort someone in a moment of sorrow when words alone cannot. This positive power of touch is countered by the potential for touch to be threatening, such as when it is connected to violence. To learn about the power of touch, we turn to haptics, which refers to the study of communication by touch (Hannaford & Okamura, 2016). People probably get more explicit advice and instruction on using touch than other nonverbal communication. A lack of nonverbal communication competence related to touch could have negative interpersonal consequences; for example, if we do not follow the advice we have been given about the importance of a firm handshake, a person might make negative judgments about our confidence or credibility. A lack of competence could have more dire negative consequences, including legal punishment if we touch someone inappropriately (intentionally or unintentionally). Touch is necessary for social development and can be welcoming, threatening, or persuasive.
There are several types of touch, including functional-professional, social-polite, friendship-warmth and love-intimacy (Heslin & Apler, 1983). At the functional-professional level, touch is related to a goal or part of a routine professional interaction, which makes it less threatening and more expected. For example, we let barbers, hairstylists, doctors, nurses, tattoo artists, and security screeners touch us in ways that would otherwise be seen as intimate or inappropriate if not in a professional context. At the socially–polite level, socially sanctioned touching behaviours help initiate interactions and show that others are included and respected. A handshake, a pat on the arm, and a pat on the shoulder are examples of social–-polite touching. A handshake is an abbreviated hand-holding gesture. Still, we know prolonged handholding would be considered too intimate and inappropriate at the functional–professional or social–polite level. Though touch still has interpersonal implications at the functional–professional, and social–polite levels. The touch between health professional and client, although professional and not intimate, has the potential to be therapeutic and comforting. In addition, a socially–polite touch exchange plays into initial impression formation, which can have important implications for how an interaction and a relationship unfold.
The need for human touch is universal in healthcare environments and is essential to the health professional–client relationship. However, multiple barriers to human touch exist in the healthcare environment. With little research to guide practice, we argue for the importance of the human touch in providing holistic care (Nist et al., 2020).
Vocalics
We learned earlier that paralanguage refers to a message’s vocalized but nonverbal parts. Vocalics is the study of paralanguage, including the vocal qualities accompanying verbal messages, such as pitch, volume and intensity, rate, vocal quality, and verbal fillers (Andersen, 1999).
Pitch
Pitch helps convey meaning, regulate conversational flow, and communicate the intensity of a message. Even babies recognize a sentence with a higher-pitched ending as a question. We also learn that greetings have a rising emphasis and farewells have a falling emphasis. Of course, no one explains these things explicitly; we learn them through observation and practice. We do not pick up on some of the more subtle and complex patterns of paralanguage involving pitch until we are older. Children, for example, have difficulty perceiving sarcasm, usually conveyed through paralinguistic characteristics such as pitch and tone rather than spoken words.
Volume and Intensity
Volume or intensity refers to how loudly or softly an individual speaks. Intensity can be tied to emotion. When individuals speak loudly, the increased volume may convey anger, emotional distress, happiness, or heightened excitement. We typically adjust our volume based on our setting, the distance between people, and the relationship. In our age of computer-mediated communication, TYPING IN ALL CAPS is usually seen as offensive, as it is equated with yelling. When individuals speak at a lower volume, the decreased volume may be an effort to diffuse an emotionally intense conversation. Lower volume could also be the result of sharing bad news, discussing taboo or sensitive topics (i.e., when people whisper “she’s pregnant” or “he died”), or conveying private information.
Rate
Speaking rate refers to how fast or slow a person speaks and can lead others to form impressions about our emotional state, credibility, and intelligence. As with volume, variations in speaking rate can interfere with the ability of others to receive and understand verbal messages. A slow speaker could bore others and cause their attention to wander. A fast speaker may be challenging to follow, and the fast delivery can distract from the message. When speaking at a faster-than-normal rate, it is essential that a speaker also clearly articulate and pronounce their words. A higher speech rate and a pleasant tone of voice can also benefit compliance gaining and aid in persuasion. Professionals must adapt their speech rate to the client’s needs in healthcare environments. A voice at a low volume or a whisper can be very appropriate when sending a covert message. Still, it would not enhance a person’s credibility if used in a professional communication context.
Tone
Our tone of voice can be controlled somewhat with pitch, volume, and emphasis, but each voice has a distinct quality known as a vocal signature. Voices vary in terms of resonance, pitch, and tone. Pitch is not generally thought about much unless an individual’s pitch stands out: a pitch at a higher or lower end of a range will be noticed if there is a momentary or situational change. For example, when children become excited or scared, they may be described as “squealing.” The situation will determine whether squealing children are thought to be excited or scared.
Verbal Fillers
Verbal fillers are sounds that fill gaps in our speech as we think about what to say next. They are considered a part of nonverbal communication because they are not like typical words that stand in for a specific meaning or meaning. Verbal fillers such as “um,” “uh,” “like,” and “ah” are common in regular conversation and are not typically disruptive. Using verbal fillers can help a person “keep the floor” during a conversation if they need to pause for a moment before continuing verbal communication. Still, for healthcare professionals, verbal fillers may communicate insecurity and a lack of confidence.
Pauses and silences are also important in creating meaning during the interaction. Pauses draw attention to important parts of messages. The “pregnant pause” is an extra-long pause that precedes particularly weighty information. Pauses are brief, but prolonged silence, such as minutes, hours, or even days, can also be used to convey meaning. Consider a professional conversation in which the client does not respond to you. What meaning is conveyed? Is the individual thinking? Is the individual hurt, angry, or too shocked to speak?
Proxemics
Proxemics refers to the study of how space and distance influence communication. We only need to look at how space is used in common metaphors to see that space, communication, and relationships are closely related. For example, when we are content with and attracted to someone, we say we are “close” to them. When we lose connection with someone, we may say they are “distant.” In general, space influences how people communicate and behave. Smaller spaces with a high density of people often lead to breaches of our personal space. Suppose this is a setting in which this type of density is expected beforehand, such as at a crowded concert or on a train during rush hour. In that case, we make various communicative adjustments to manage the space issue. Unexpected breaches of personal space can lead to adverse reactions, especially if we feel someone has violated our space voluntarily, meaning that a crowding situation did not force them into our space. Additionally, research has shown that crowding can lead to criminal or delinquent behaviour, known as a “mob mentality” (Andersen, 1999). To better understand how proxemics function in nonverbal communication, we will more closely examine the proxemic distances associated with personal space and the concept of territoriality.
Proxemic Distances
We all have varying definitions of our “personal space”; these definitions are contextual and depend on the situation and the relationship. Although our “bubbles” are invisible, people are socialized into the norms of personal space within their cultural group. Hall (1968) identified four zones: public, social, personal, and intimate distance. The zones are more elliptical than circular, taking up more space in front of us, where our line of sight is than at our side or back, where we cannot monitor what people are doing. The figures below show how these zones relate to each other and the individual. Even within a particular zone, interactions may differ depending on whether someone is in the outer or inner part of the zone.
Public Space (3 Metres/12 feet+ or More)
Public space starts about three and a half metres (twelve feet) from a person and extends from there.
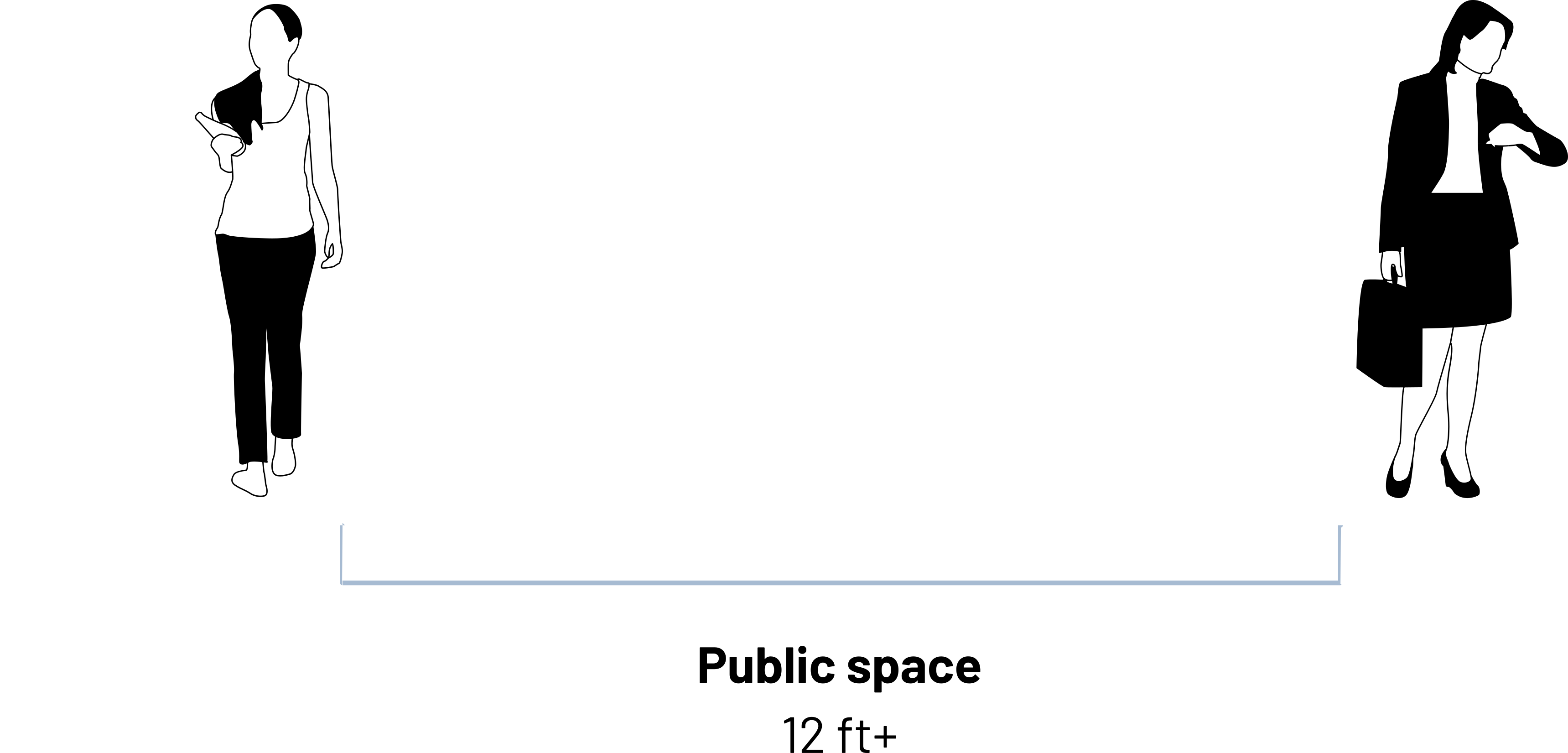
This is the least personal of the four spaces and would typically be used when a person is engaging in a formal speech or when a high-profile or influential person such as a celebrity or executive maintains such a distance as a sign of power or for safety and security reasons. Regarding regular interaction, we are often not obligated or expected to acknowledge or interact with people who enter our public zone. It would be challenging to have a deep conversation with someone at this level because one would have to speak loudly, and there is no physical closeness that is often needed to promote emotional closeness or establish rapport.
Social Space (1–3 Metres/4-12 feet)
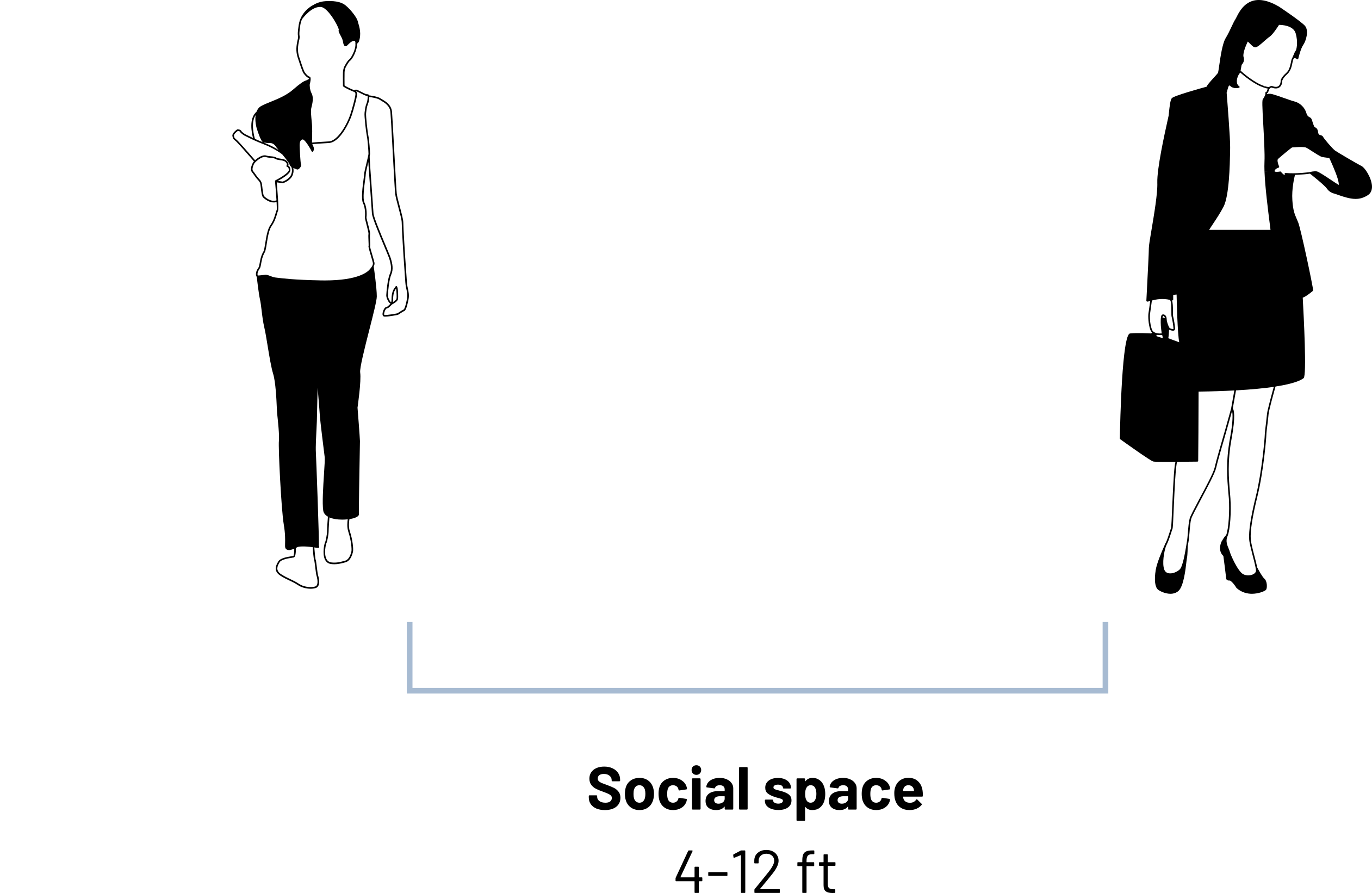
Communication in the social space is one to three metres (about four to twelve feet) away from our body, is typical in professional or casual interactions but is neither intimate nor public. This distance is preferred in many professional settings. It is possible to have people in the outer portion of this social zone but not feel obligated to interact with them. Still, when people come closer than two metres to us, we often feel obligated to at least acknowledge their presence.
Personal Space (1.5 meters/0-4 feet or Less)
Personal and intimate space start at our physical body and extend about a metre (three to four feet).
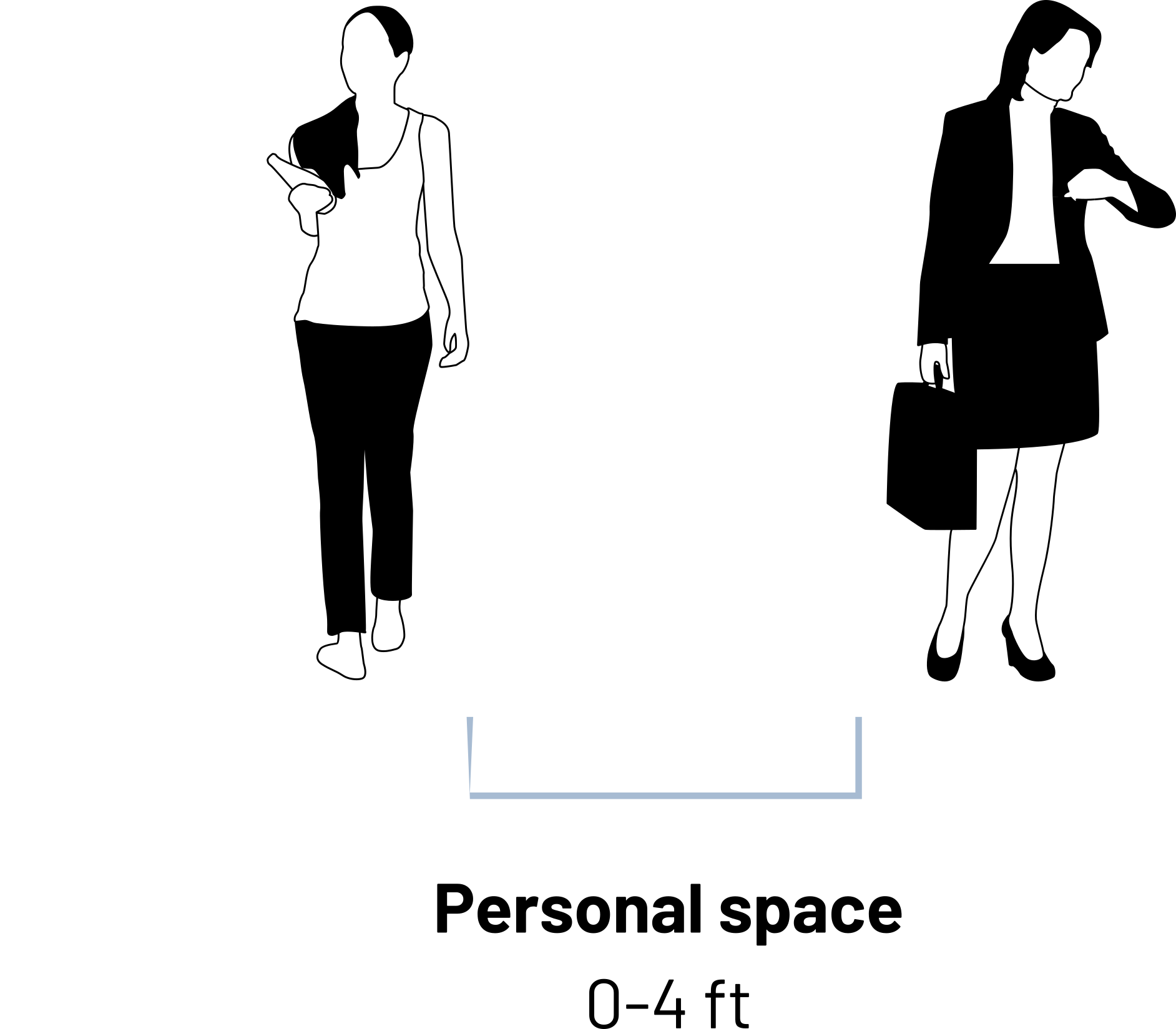
Much of our communication occurs in the personal zone, which we typically consider our “personal space bubble,” and extends from less than a metre to a little more than a metre (one-and-a-half feet to four feet) away from our body. Even though we are getting closer to the physical body of another person, we may use verbal communication at this point to signal that our presence in this zone is friendly and not intimate. Even people who know each other well could be uncomfortable unnecessarily spending too much time in this zone. This zone is broken into two subzones, which helps us negotiate close interactions with people we may not be close to interpersonally (McKay et al., 1995, p. 59). The outer-personal zone extends from nearly a metre to slightly more than a metre away (tow-and-a-half feet to four feet). It is helpful for conversations that need to be private but between people who are not interpersonally close. This zone allows for intimate communication but does not convey the intimacy that a closer distance would, which can be beneficial in professional settings. The inner-personal zone extends less than a metre (one-and-a-half to two-and-a-half feet). It is a space reserved for communicating with people we are interpersonally close, trying to get to know, or with health professionals. In this subzone, we can easily touch the other person as we talk to them, briefly placing a hand on his or her arm or engaging in another light social touching that facilitates conversation, empathy, self-disclosure, and feelings of closeness.
Intimate Space (Less than 1 Metre/0-1.5 feet)
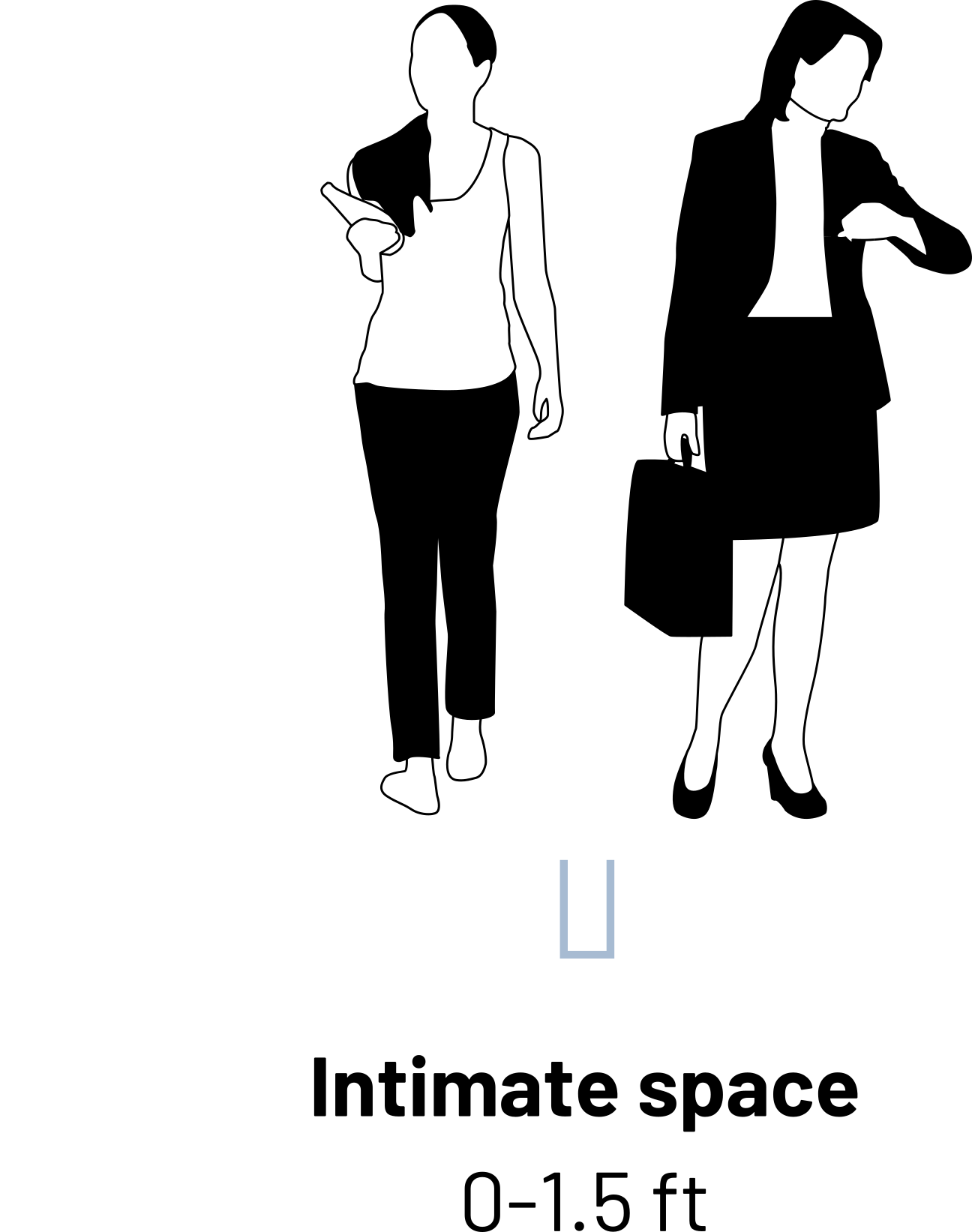
As we breach the invisible line that is a metre or less (one-and-a-half feet) from our body, we enter the intimate space, reserved for only the closest friends, family, romantic or intimate partners, and some health professionals. It is impossible to completely ignore people when they are in this space, even if we are trying to pretend that we are ignoring them. A breach of this space can be comforting in some contexts and annoying or frightening in others. We need regular human contact that is not just verbal but also physical. We have already discussed the importance of touch in nonverbal communication, and for that much-needed touch to occur, people must enter our intimate space. Being close to someone and feeling their physical presence can be very comforting when words fail. There are also social norms regarding the amount of this type of closeness that can be displayed in public, as some people become uncomfortable even seeing others interacting in the intimate zone. While some people are comfortable engaging in or watching others in PDAs (public displays of affection), others are not.
So what happens when our space is violated? Although these zones are well established in research regarding the personal space preferences of Canadians (McKay et al., 1995), individuals vary in terms of their reactions to others entering certain zones, and determining what constitutes a “violation” of space is subjective and contextual. For example, another person’s presence in our social or public zones does not typically arouse suspicion or adverse physical or communicative reactions, though it might in some situations or with certain people. However, many situations lead to our personal and intimate space being breached by others against our will. These breaches are more likely to be upsetting, even when expected. We have all had to get into a crowded elevator or wait in a long line. In such situations, we may rely on some verbal communication to reduce immediacy and indicate that we are not interested in closeness and are aware that a breach has occurred. People may comment about the crowd, such as, “We are packed in here like sardines,” or use humour to indicate that they are pleasant, well-adjusted, and uncomfortable with the breach like any “normal” person would be. Interestingly, as we will learn in our discussion of territoriality, we do not often use verbal communication to defend our personal space during regular interactions. Instead, we rely on more nonverbal communication, such as moving, crossing our arms, or avoiding eye contact to deal with space breaches. It is also essential to be aware of your professional practice standards and what is considered professional and unprofessional conduct. Take the time to locate and review practice standards applicable to your profession.
Territoriality
Territoriality is an innate drive to take up and defend spaces. This drive is shared by many creatures and entities, ranging from packs of animals to individual humans to nations. Whether it is a neighbourhood claimed by a particular salesperson, your preferred place to sit in a restaurant, your usual desk in the classroom, or the seat you have marked to save while getting concessions at a sporting event, we claim specific spaces as our own. Territory has three main divisions: primary, secondary, and public (Hargie, 2011, p. 70). Sometimes our claim to a space is official. These spaces are our primary territories because they are marked or understood as exclusively ours and under our control. A person’s house, yard, room, desk, side of the bed, or shelf in the medicine cabinet could be considered primary territory.
Secondary territories do not belong to us and are not exclusively under our control. Still, they are associated with us, which may lead us to assume that the space will be open and available to us when we need it without taking further steps to reserve it. This happens in classrooms regularly. Students often sit at the same desk or at least the same general area as they did on the first day of class.
Public territories are open to all people. People can mark public territory and use it for a limited period, but space is often up for grabs, making it challenging for some people to manage and can lead to conflict. To avoid this situation, people use a variety of objects typically recognized by others as nonverbal cues that mark a place as temporarily reserved — for example, jackets, bags, papers, or a drink.
Chronemics
Chronemics refers to the study of how time affects communication. Time can be classified into several categories, including biological, personal, physical, and cultural (Andersen, 1999). Biological time refers to the rhythms of living things. Humans follow a circadian rhythm, meaning that we are on a daily cycle that influences eating, sleeping, and waking. Our physical and mental health, communication competence, and personal relationships can suffer when our natural rhythms are disturbed, such as by all-nighters or jet lag. Keep biological time in mind as you communicate with others. Remember that early morning conversation and speeches may require more preparation to be awake enough to communicate well. A more patient or energetic delivery may be needed to accommodate others who are still warming up for their day.
Personal time refers to how individuals experience time (Bruneau, 2011). How we experience time varies based on our mood, interest level, and other factors. Think about how quickly time passes when you are interested in and therefore engaged in something. We have been in 80-minute classes that seemed to drag on forever and three-hour classes that zipped by. Individuals also vary based on whether or not they are future- or past-oriented. People with past-time orientations may want to reminisce, reunite with old friends, and spend considerable time preserving memories and keepsakes in scrapbooks and photo albums. People with future-time orientations may spend the same time making career and personal plans, writing to-do lists or researching future vacations, potential retirement spots, or the book they plan to read next.
Physical time refers to the fixed cycles of days, years, and seasons. Physical time, especially seasons, can affect our mood and psychological states. Some people experience seasonal affective disorder that leads them to experience emotional distress and anxiety during the changes of seasons, primarily from warm and bright to dark and cold (summer to fall and winter).
Cultural time refers to how a large group of people views time. Polychronic people do not view time as a linear progression that needs to be divided into small units and scheduled in advance. Polychronic people keep more flexible schedules and may engage in several activities simultaneously. Monochronic people schedule their time more rigidly and do one thing at a time. A polychronic or monochronic orientation to time influences our social realities and interactions with others.
Additionally, how we use time depends in some ways on our status. For example, doctors can make their patients wait for extended periods, and executives and celebrities may be consistently behind schedule, making others wait for them. Promptness and the amount of socially acceptable time for lateness and waiting varies among individuals and contexts. Chronemics also includes the amount of time we spend talking.
Personal Presentation and Environment
Personal presentation involves our physical characteristics and the artifacts we adorn and surround ourselves with. Physical characteristics include body shape, height, weight, attractiveness, and other physical features. We do not have as much control over how these nonverbal cues are encoded as we do with many other aspects of nonverbal communication. These characteristics play a significant role in initial impression formation, even though we know we “should not judge a book by its cover.” Although ideals of attractiveness vary among cultures and individuals, research consistently indicates that people deemed attractive based on physical characteristics have distinct advantages in many aspects of life. This fact and media images often project unrealistic beauty ideals, contributing to booming health and beauty, dieting, gym, and plastic surgery industries.
Have you ever tried to change your conscious “look?” Simple clothing changes can impact how people are perceived. Aside from clothes, jewelry, visible body art, hairstyles, and other political, social, and cultural symbols send messages to others about who we are. Body piercings and tattoos have shifted from subcultures to the mainstream over the past few decades. The physical location, size, and several tattoos and piercings play a significant role in whether or not they are appropriate for professional contexts. Many people with tattoos or piercings make conscious choices about when and where they display their body art. Hair also sends messages, whether it is on our heads or our bodies. Men with short hair are generally considered more conservative than men with long hair, but men with shaved heads may be seen as aggressive. Whether a person has a part in their hair, a mohawk, faux-hawk, ponytail, curls, or bright pink hair also sends nonverbal signals to others.
Jewelry can also send messages with varying degrees of direct meaning. In North America, a ring on the “ring finger” of a person’s left hand typically indicates that they are married or in an otherwise committed relationship; a thumb ring or a right-hand ring on the “ring finger” does not send such a direct message. People also adorn their clothes, body, or belongings with religious or cultural symbols, such as a cross to indicate a person’s Christian faith or a rainbow flag to indicate that a person is gay, lesbian, bisexual, transgender, queer, or an ally to one or more of these groups.

Lastly, the environment in which we interact affects our verbal and nonverbal communication because we can often manipulate the environment, similar to how we would manipulate our gestures or tone of voice to suit our communicative needs. The books we display on our coffee table, the magazines a doctor keeps in their waiting room, the placement of fresh flowers in a foyer, or a piece of mint chocolate on a hotel bed pillow all send particular messages and can be easily changed. Placing objects and furniture in a physical space can help create a formal, distant, friendly, or intimate climate. In formality, we can use nonverbal communication to convey dominance and status, which helps define and negotiate power and roles within relationships. A room with soft lighting, a small fountain that creates the ambient sound of water flowing, and a comfortable chair can help facilitate interactions between a therapist and a client. In summary, whether we know it or not, our physical characteristics and artifacts communicate messages with the world around us.
View the two videos below, and refer to the questions that follow.
Watch: Clinical communication skills
Video Transcript (see Appendix B 4.2.1)
Video Transcript (see Appendix B 4.2.2)
- What are some differences in nonverbal communication you observed while watching the videos? What nonverbal communication skills could you utilize in your professional interactions?
- Have you experienced a similar interaction? How did it make you feel? What could have been done differently if you could experience it again?
Key Takeaways
-
Kinesics refers to body movements and posture and includes the following components:
- Gestures are arm and hand movements and include adaptors such as clicking a pen or scratching your face, emblems such as a thumbs-up to say “OK,” and illustrators such as bouncing your hand along with the rhythm of your speech.
- Head movements and posture include the orientation of movements of our head, the orientation and positioning of our body, and the various meanings this sends. Head movements such as nodding indicate agreement, disagreement, and interest, among other things. Posture can indicate assertiveness, defensiveness, interest, readiness, or intimidation, among other things.
- Eye contact is studied under the category of oculesics and refers explicitly to eye contact with another person’s face, head, and eyes, and the patterns of looking away and back at the other person during the interaction. Eye contact provides turn-taking signals, indicates that we are engaged in cognitive activity, and helps establish rapport and connection, among other things.
- Facial expressions refer to using the forehead, brow, and facial muscles around the nose and mouth to convey meaning. Facial expressions can convey happiness, sadness, fear, anger, and other emotions.
- Haptics refers to touch behaviours that convey meaning during interactions. Touch operates at many levels, including functional–professional, social–polite, friendship–warmth, and love–intimacy.
- Vocalics refers to the vocalized but not verbal aspects of nonverbal communication, including our speaking rate, pitch, volume, tone of voice, and vocal quality. These qualities reinforce the meaning of verbal communication, allow us to emphasize particular parts of a message, or can contradict verbal messages.
- Proxemics refers to the use of space and distance within communication. North Americans, in general, have four spaces that constitute our personal space: public space (3-4 metres/12 feet or more from our body), social space (around 1 to 4 metres/4–12 feet from our body), personal space (half a metre to a metre/1.5–4 feet from our body), and intimate space (from body contact to half a metre/1.5 feet away). Proxemics also studies territoriality, or how people take up and defend personal space.
- Chronemics refers to the study of how time affects communication. It includes how different time cycles affect our communication, including differences between past- or future-oriented people and cultural perspectives on time as fixed and measured (monochronic) or fluid and adaptable (polychronic).
- Personal presentation and environment refer to how the objects we adorn ourselves and our surroundings (artifacts) provide nonverbal cues from which others make meaning and how our physical environment — for example, the layout of a room and seating positions and arrangements — influences communication.
Exercises
- Provide examples of how eye contact plays a role in your daily communication.
- The Covid-19 pandemic has created new challenges regarding the use of therapeutic touch. What types of touch might be present or used within healthcare environments? How have social distancing and infection control practices impacted therapeutic touch within healthcare environments? What are your feelings about therapeutic touch? What are your feelings about social distancing? How might these feelings affect your interactions with others within a healthcare environment?
- How do you think wearing COVID-19 PPE (personal protective equipment) might impact your ability to recognize nonverbal cues within your professional role? How might it impact your client’s or their family’s ability to recognize your nonverbal cues?
- Many people do not consider time an essential part of our nonverbal communication. Consider an example of how chronemics sends nonverbal messages in academic, professional, and personal settings.
References
Adler, R., Rosenfeld, L. B., & Proctor, R. F., II. (2013). Interplay: The process of interpersonal communication. Oxford.
Andersen, P. A. (1999), Nonverbal communication: Forms and functions. Mayfield.
Bruneau, T. (2011). Chronemics and the verbal-nonverbal interface. In The relationship of verbal and nonverbal communication (pp. 101-118). De Gruyter Mouton. https://doi.org/10.1515/9783110813098.101
Evans, D. (2011). Emotion: The science of sentiment. Oxford University Press.
Hall, E. T. (1968). Proxemics. Current Anthropology 9(2), 83–95.
Hannaford, B., & Okamura, A. M. (2016). Haptics. In Springer handbook of robotics (pp. 1063-1084). Springer, Cham. https://doi.org/10.1007/978-3-319-32552-1_42
Hargie, O. (2011). Skilled interpersonal interaction: Research, theory, and practice (5th ed.). Routledge.
Harrigan, J. A. (2005). Proxemics, kinesics, and gaze. In J. A. Harrigan, R. Rosenthal, & K. R. Scherer (Eds.), The new handbook of methods in nonverbal behavior research (pp. 137–198). Oxford University Press.
Heslin, R., & Apler, T. (1983). Touch: A bonding gesture. In J. Weimann & R. Harrison (Eds.), Nonverbal interaction (pp. 47–76). SAGE.
Martin, J. N., & Nakayama, T. K. (2010). Intercultural communication in contexts (5th ed.). McGraw-Hill.
McKay, M., Davis, M., & Fanning, P. (1995). Messages: Communication skills book (2nd ed.). New Harbinger Publication.
Nist, M., Harrison, T. M., Tate, J., Robinson, A., Balas, M., & Pickler, R. H. (2020). Losing touch. Nursing Inquiry, 27(3). https://doi.org/10.1111/nin.12368
Pease, A., & Pease, B. (2004). The definitive book of body language. Bantam.
Stickley, T. (2011). From SOLER to SURETY for effective non-verbal communication. Nurse Education Practice, 11(6), 395-8. https://doi.org/10.1016/j.nepr.2011.03.021
Image Attributions
Figure 4.2.1. Thumbs Up by Kreg Steppe. Licensed under CC BY-SA 2.0.
Figure 4.2.2 Public space. Kindred Grey. 2022. CC BY 4.0. Includes Person by mungang kim from NounProject and Person by mungang kim from NounProject (both NounProject license).
Figure 4.2.3. Social space. Kindred Grey. 2022. CC BY 4.0. Includes Person by mungang kim from NounProject and Person by mungang kim from NounProject (both NounProject license).
Figure 4.2..4. Personal space. Kindred Grey. 2022. CC BY 4.0. Includes Person by mungang kim from NounProject and Person by mungang kim from NounProject (both NounProject license).
Figure 4.2..5. Intimate space. Kindred Grey. 2022. CC BY 4.0. Includes Person by mungang kim from NounProject and Person by mungang kim from NounProject (both NounProject license).
Figure 4.2..6. My desk by Phil Stripling. Licensed under CC BY-NC 2.0.
Media Attributions
TED. (2012). Your body language shapes who you are [Video]. Cuddy, A. (Speaker), Geni, J. (Translator), Bast, M. (Reviewer). https://www.youtube.com/watch?v=Ks-_Mh1QhMc
University of Nottingham. (2014, June 30). Clinical communication skills – Non-verbal communication consultation – version 1 of 2 [Video]. YouTube.
University of Nottingham. (2014, June 30). Clinical communication skills – Non-verbal communication consultation – version 2 of 2 [Video]. YouTube. https://www.youtube.com/watch?v=-1Ba9juSMfM&t=10s
Attribution Statement
Content adapted, with editorial changes, from:
University of Minnesota Libraries Publishing. (2013). Communication in the real world [Adapted]. https://open.lib.umn.edu/communication/
Wrench, J. S., Punyanunt-Carter, N., & Thweatt, K. S. (n.d.). Interpersonal communication: A mindful approach to relationships. Milne Library Publishing.
Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License, except where otherwise noted.

